The Nonverbal Escalation Continuum

Dustin Hoffman in his role as Raymond Babbet, an autistic savant, in the award-winning movie "Rainman," has brought a great deal of attention to the severe developmental disorder of autism. The film has heightened public awareness of the puzzling condition and the social, behavioral and communicative difficulties experienced by people with autism.
Kerry's Place is an agency in Ontario, Canada which provides residential and outreach support services to individuals having autism. The goal of the organization is to assist children and adults with autism to develop practical living skills, social skills, socially acceptable behavior, and a functional means of communicating. Approximately 50% of the autistic population is nonverbal. For many, the frustration with their communication disorder has resulted in the development of behavior problems, attention seeking, self-injurious or aggressive behaviors.
Training in crisis prevention has provided Kerry's Place staff with methods of preventing, intervening and diffusing many behavioral outbursts. One of the key elements discussed in the CPI preventative techniques is the recognition of the verbal escalation continuum and the corresponding staff responses. Staff working with individuals with autism have frequently identified the need to recognize a similar escalation continuum for their clients who are nonverbal. Investigation has revealed that indeed the same process occurs in an observable nonverbal means in those people who cannot communicate verbally. As a result, the Nonverbal Escalation Continuum for persons with developmental handicaps and autism has been developed following a similar paradigm.
The nonverbal person with autism is afflicted with a severe communication disorder, limiting both expressive and receptive communication skills. A difficulty comprehending verbal language and the inability to learn through verbal rationalization and explanation is common. Autistic individuals may be characterized as experiential learners. This learning style means teaching must take place through concrete experience at the time of use, especially when teaching communication skills. The experiential learner also has difficulty generalizing information from one experience to another. If skills are not taught in context, they will not necessarily be associated with the correct usage. This has important implications for staff responding to the nonverbal escalation continuum. Unlike the general population, who can learn from their experience during the tension reduction stage via therapeutic rapport, the experiential learner must practice new skills at the time of need.
The observable behaviors demonstrated in the anxiety stage by the nonverbal population with autism must be interpreted as sincere attempts to communicate by a person who may have no other means of doing so. Responding to the general population experiencing anxiety requires a supportive caring attitude. However, in responding to demonstrated anxiety in a nonverbal person with autism, the staff response needs to be more than simply supportive. Just being there and caring will not help nonverbal persons communicate what they are feeling at the time or learn a more effective means of doing so.
The intervention for this stage is interpret and teach. In this intervention, reflect behaviors back to the individual and attempt to interpret the meaning of the behaviors. Next, try to teach the individual a way of communicating the message more effectively; e.g., Interpreting: "You're shaking your arms and you're frowning...you look angry." "You're pointing to the kitchen...you want me to see something in the kitchen." Teaching: "Relax, I understand you. Take my hand and lead me to the kitchen...show me what you want."
Anxiety behaviors and nonverbal attempts to communicate will resurface frequently throughout the continuum. During the early stages of the continuum, interveners must be cognizant of the experiential learning style and use these concrete opportunities to teach ways of communicating.
Consideration should be given to augmentative communication systems for nonverbal individuals. Written word, sign language, gestures, photographs, and pictorial symbols are all useful tools for aiding expressive communication for the nonverbal person with autism. These experiential learners need to experience immediate results and rewards for their attempts to communicate with any of the above systems. It is only by reinforcement during concrete experience that they understand the value and power of communication.
Interveners can aid receptive communication skills and comprehension by augmenting their own communication with any of the aforementioned communication systems.
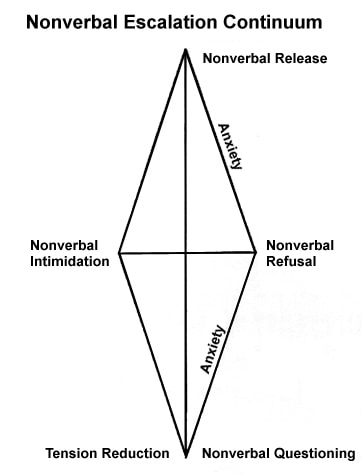
Nonverbal Questioning
Questioning may take two different forms with the nonverbal population.:
-
The first is a need for clarification. The individual may not have understood the request or may not have had time to process the information. This may manifest itself in nonresponsiveness, eye contact or lack of eye contact; they may walk away or seem distracted.
Intervention - It is important to allow enough time for the individual to process the information as well as clarifying your request. Use augmentative communication systems to enhance the client's level of understanding (i.e., sign language, pictorial communication symbols). -
The second form of questioning is avoidance. The individual does not want to do the task so may walk away or request the washroom in an attempt to avoid the task. It is important to realize that this is a type of power struggle and must be dealt with as such.
Intervention - It is important to give choices; e.g., first we'll do this, then we'll do that, set limits and keep the individual on topic. Avoid a power struggle as this may escalate the situation. With the resurfacing of anxiety, respond by interpreting and teaching in response to the experiential learner's style; e.g., alternatives to task avoidance, requesting or signing "break, please," negating, and reinforce this.
Nonverbal Refusal
In the area of refusal, the individual will become noncompliant; they may walk away or sit down in a very matter of fact fashion. There may be extreme eye contact, or no eye contact at all, depending on the individual.
Intervention - Be proactive by interpreting the behavior and teaching alternatives. Ensure that the choices are clear and simple. Reclarify the request and allow time for processing. Continue to use positive limits. All limits should be reasonable and enforceable.
Nonverbal Release
During release the behaviors exhibited by a nonverbal individual may take the form of self-injurious behavior (SIB); i.e., head banging, biting, slapping. They may exude noises; screaming, crying. There may also be some tantrum behavior; stomping feet, banging walls or throwing objects. In this stage, the energy output is extremely high and there is no apparent focus.
Intervention - It is imperative that all other clients are removed from the area to prevent a behavioral chain reaction from occurring (contagion). If possible allow venting (excluding any SIB or aggressive behavior). In a calming fashion, using augmented communication systems (sign language, PCS), state the directive in a nonthreatening fashion. Remember your tone, volume and cadence. Allow more time for the processing of the information to occur. The focus is to have the individual regain control before continuing with the original request or the setting of limits.
The levels of release and intimidation may be difficult to differentiate with the nonverbal population, thus it is imperative to be prepared during the release stage with a back-up plan of action in the event that a physical threat becomes apparent.
Nonverbal Intimidation
The signs of agitation; e.g., facial expressions, grimaces, hyperactivity, and any one of the behaviors exhibited during release, can quickly lead to a true physical threat as previously mentioned.
Intervention - It is important to have a plan of action for each individual prior to an event occurring. This allows for the situation to be handled smoothly, ensuring the care, welfare, safety, and security of everyone involved. It is important to remember that the processing time is critical when dealing with a nonverbal individual. Be patient. Use nonviolent physical crisis intervention techniques as a last resort in dealing with someone who is physically out-of-control.
Tension Reduction
The tension reduction stage is often a difficult time for the nonverbal person with autism. Feelings of sorrow, shame and regret have no outlet by way of communication with the others involved. Comfort during and following tension reduction is often drawn from a return to familiar and positive activities and routines where praise and approval are the norm.
The tension reduction stage is also a difficult stage for the intervener. Although the intervener wants to comfort and support, he or she must also recognize important elements of the experiential learning style. A behavior escalation which resulted in acting-out behavior followed immediately by a great deal of attention and positive reward may inadvertently reinforce the acting-out behavior; i.e., the experiential learner has experienced "when I yell and hit then I get attention and praise."
It is especially important in working with the experiential learner that requests, limits and consequences are consistent and concrete. Following tension reduction, the intervener must ensure that the behavior escalation has not been reinforced by eliminating the original request, limit or consequence.
The intervener may try to explain what was unacceptable and why. The intervener may also reassure the client that he or she can do better next time. Trying to teach new skills at this stage will seldom generalize to use in a future crisis event.
Summary Comments
Effective intervention with nonverbal individuals with autism must include the recognition of behaviors as sincere attempts to communicate. Interveners must learn to interpret behaviors and attempt to teach alternative means of communicating. Attempts to teach improved modes of communication must take into consideration the experiential learning style of individuals with this communication disorder. Finally, interveners must recognize the five stages of the escalation continuum as experienced by nonverbal individuals with autism and learn to respond accordingly - this will enable them to provide for the care, welfare, safety, and security of all involved.
Susan Repa and Neil Walker, Kerry's Place
National Report -- Fall 1990 -- Volume 10, Number 2
Schedule a Consultation
Learn how CPI’s training programs can benefit your organization.
Let's Connect